
TL;DR
- Medical canvassing contacts healthcare facilities directly to confirm whether a claimant received treatment, and if so, when and where, without requesting full clinical records.
- A canvass returns treatment dates and locations, provider identity and NPI numbers, prior claims history, and pharmacy pickup records. It does not return charts, diagnoses, or billing detail.
- Order one early when a claimant reports little prior treatment, when dates don't match the reported history, or when statements raise inconsistencies.
- A rigorous vendor delivers documented, auditable responses across a broad facility radius. A commodity provider hands you a verbal confirmation you can't defend later.
What Medical Canvassing Is (and What It Is Not)
Medical canvassing is the practice of contacting hospitals, clinics, and pharmacies directly to confirm whether a claimant received treatment, and when and where it occurred. The core question a canvass answers stays narrow. Did treatment occur, and if so, when and where? CDI Canvassing frames the practice around exactly that question, and the precision matters because it defines both the value and the legal footing of the work (CDI Canvassing).
A canvass operates as a desktop investigation that surfaces only non-protected details. Alpine Intel describes canvassers confirming treatment facts within the boundaries of HIPAA, which protects sensitive health data from disclosure without patient consent (Alpine Intel). Confirming that a visit happened on a given date at a named facility falls outside protected clinical content, so no medical release is required to ask. That distinction is why a canvass can move quickly while a records request waits on authorization.
The cleanest way to understand canvassing is to set it against medical records retrieval. Records retrieval pulls full charts, billing statements, and clinical documentation, and it depends on a signed release. Canvassing asks none of that. It verifies the existence and timing of treatment, not its substance, and it stops short of anything inside the chart.
That boundary shapes everything else in a canvassing program. It determines what an adjuster can order without authorization, what a canvass can return, and when the results justify escalating to a subpoena or a full records request. The rest of this guide builds on that line.
What a Medical Canvass Actually Returns
A medical canvass returns a defined set of confirmation facts, not a clinical summary. Alpine Intel's output list maps closely to what most rigorous canvasses produce. You should expect treatment location, the reported date of injury, a timeline of events, and a determination of whether a given injury connects to the claim under review. A canvass also surfaces previous treatments for similar injuries and a history of prior claims, which is often the finding that changes how an adjuster weighs a file.
The canvass also captures each facility's National Provider Identifier, the NPI number that ties a confirmed treatment record to a specific provider. That identifier matters downstream. When you later issue a subpoena or request full records, the NPI removes ambiguity about which facility you are pursuing.
Pharmacy canvassing widens the picture beyond the treating facility. Canvassers contact pharmacies within a geographic radius of where the claimant lives or where the injury occurred, and they confirm which medications were prescribed, when, and whether and when the claimant actually picked them up. A prescription that was written but never filled tells a different story than one filled on schedule, and that gap is the kind of detail a canvass exists to find.
Facility scope determines how complete the output is. A canvass that touches only hospitals will miss treatment that happened at urgent care, walk-in clinics, or specialty practices. The vendors that return the most usable results define a wide enough net up front, covering hospitals, urgent care, specialty clinics, and pharmacies across the relevant radius. When you order a canvass, ask what facility types and geographic range the vendor will actually canvass, because that scope sets the ceiling on what you can learn.
How Medical Canvassing Works: The Step-by-Step Process
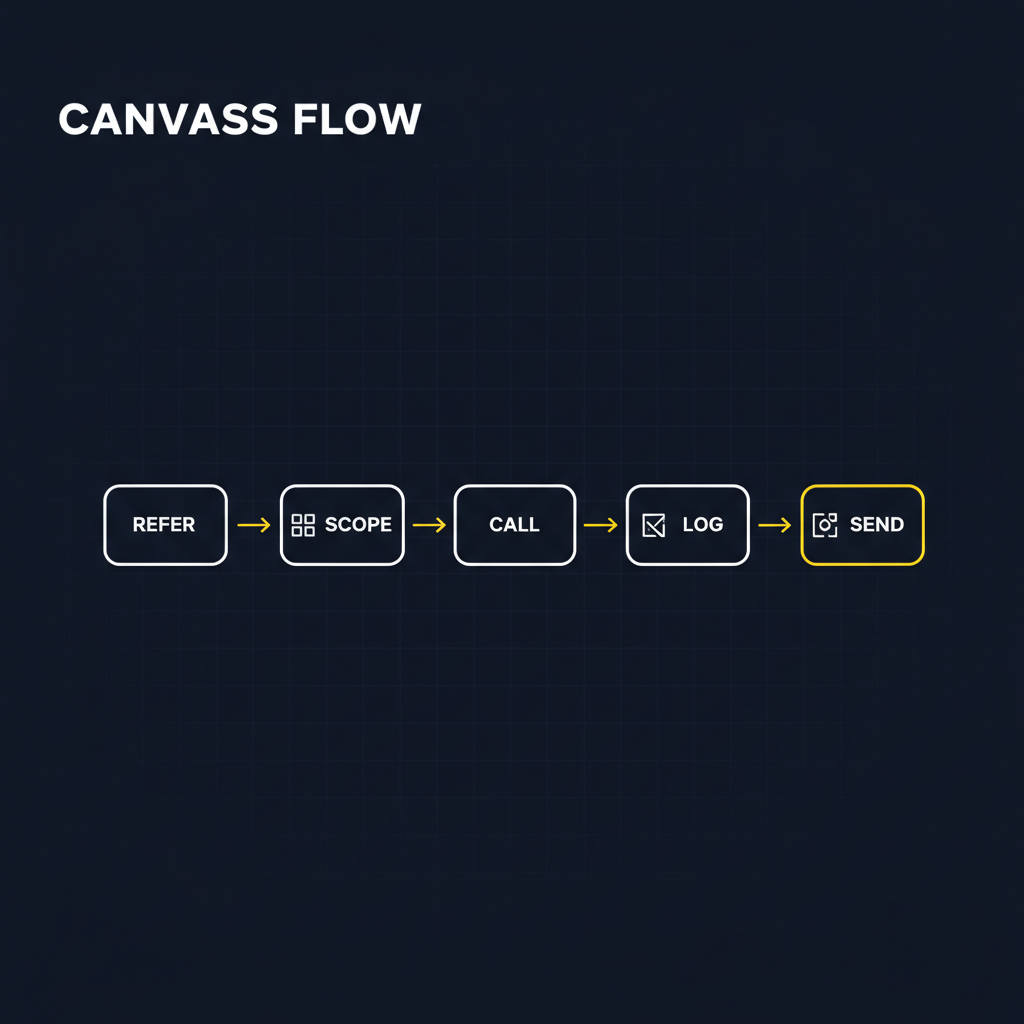
A medical canvass starts with a referral, usually from a claims adjuster or SIU analyst who has a reason to question a treatment history. The referral carries the inputs that drive everything downstream: the claimant's name, date of birth, the reported date and location of injury, and any provider names already on file. Thin referral data produces a weaker canvass, so the quality of what you submit shapes the quality of what you get back.
Scoping comes next, and it determines hit rate more than any other step. The vendor maps a geographic radius around where the claimant lives and where the injury allegedly occurred, then builds a target list of facilities inside that radius. Alpine Intel's facility scope is a useful reference here, covering hospitals, urgent care and walk-in clinics, specialty clinics, and pharmacies within the radius (Alpine Intel). A canvass that omits pharmacies misses medication pickup records, and one with a tight radius misses providers a claimant traveled to.
Outreach is the part that consumes labor. Canvassers contact each facility on the list and ask whether the claimant was treated, and if so, on what dates and by which provider. Every facility is a separate phone call or fax, and a single claim can involve dozens of contacts across the radius. Facilities respond on their own timeline, so a canvass against fifty providers runs as fifty parallel inquiries that resolve at different speeds.
Logging is where rigor separates a usable canvass from an anecdote. Each response gets recorded as a confirmed treatment, a confirmed negative ("no record of this patient"), or an unresolved contact still pending a callback. The negatives matter as much as the hits, because a documented "no treatment" at every facility in the radius is itself an evidentiary finding. A verbal confirmation a canvasser remembers from a phone call is not. What makes a result defensible later is a written, timestamped record of who was contacted, when, and what they said.
The final step is delivery of a documented report that lists every facility contacted, the response from each, and the dates and provider details that came back. An auditable trail is what lets a downstream subpoena, surveillance referral, or claim denial stand on the canvass. If you cannot show your work facility by facility, the findings won't survive scrutiny when the claim is contested.
What Triggers a Medical Canvass Referral

Three claim patterns justify ordering a canvass, and Alpine Intel groups them by how much suspicion they carry. The trigger type tells you when to order, not just whether to.
Subjective injury claims top the list because they leave little to verify on their own. Soft-tissue complaints turn on reported pain rather than imaging or measurable findings, so an adjuster has no independent way to confirm a doctor was ever seen. A canvass answers the basic question of whether and when the claimant sought treatment, which is exactly the gap a soft-tissue claim leaves open. Order these early, before the file accumulates assumptions built on the claimant's account alone.
Claimant memory gaps trigger a canvass for reasons that have nothing to do with suspicion. When the insured cannot recall provider names, appointment dates, treatment length, or medication names, Alpine Intel frames the resulting referral as fact-finding alone. You are filling in a record the claimant genuinely cannot supply, not testing their honesty. Treat these as routine reconstruction work and order them as soon as the gap surfaces in a statement.
Suspicion of misrepresentation is the third trigger, and it carries the most weight. Indicators like a claimant avoiding or refusing diagnostic procedures can signal malingering, which Alpine Intel defines as prolonging or exaggerating symptoms of a real injury. A referral here does not presume guilt. A canvass can just as easily confirm no wrongdoing and clear the file. The point is that the inconsistency itself, not the adjuster's hunch, is what the canvass tests.
Across all three, timing decides how much the result is worth. CDI Canvassing argues that the earlier a canvass runs, the more it shapes claim direction, because findings that arrive before the file hardens prevent downstream rework, delays, and decisions made on incomplete history. A canvass ordered after surveillance and authorizations are already in motion often confirms what later steps could have skipped. Tie the referral to the trigger and run it early.
What Medical Canvassing Can and Cannot Ask Under HIPAA
A medical canvass operates inside HIPAA, not around it. The reason no patient authorization is required comes down to what a canvasser asks for. A canvass confirms that a treatment event happened. It does not request the clinical substance of that treatment, and that distinction is what keeps the inquiry compliant.
The details a canvass can confirm fall outside HIPAA's protected zone. A canvasser can verify the date of an injury, the identity and National Provider Identifier of a facility, whether a claimant was treated there, and the timeline of visits. A pharmacy canvass can confirm that a medication was prescribed and picked up on a given date. None of these answers reveal a diagnosis, a chart note, or the content of a physician's assessment. They establish the existence and timing of care, which is precisely the question an SIU team needs answered.
The protected material is everything HIPAA was written to guard. Diagnoses, treatment plans, test results, and clinical records require a signed medical authorization, a subpoena, or another lawful release before any provider hands them over. A canvasser who tries to extract that content has crossed the line and exposed the claim to a privacy violation. A competent vendor trains its outreach staff to stop at confirmation and escalate when the answer requires a release.
Reading canvassing as a privacy workaround is the most common misconception, and it gets the practice backwards. A canvass is a defined inquiry type with a fixed scope, not a shortcut past consent rules. As Alpine Intel frames it, every detail surfaced must comply with HIPAA. The compliance is built into what the inquiry is allowed to ask.
Where Canvassing Fits in the Broader SIU Investigation
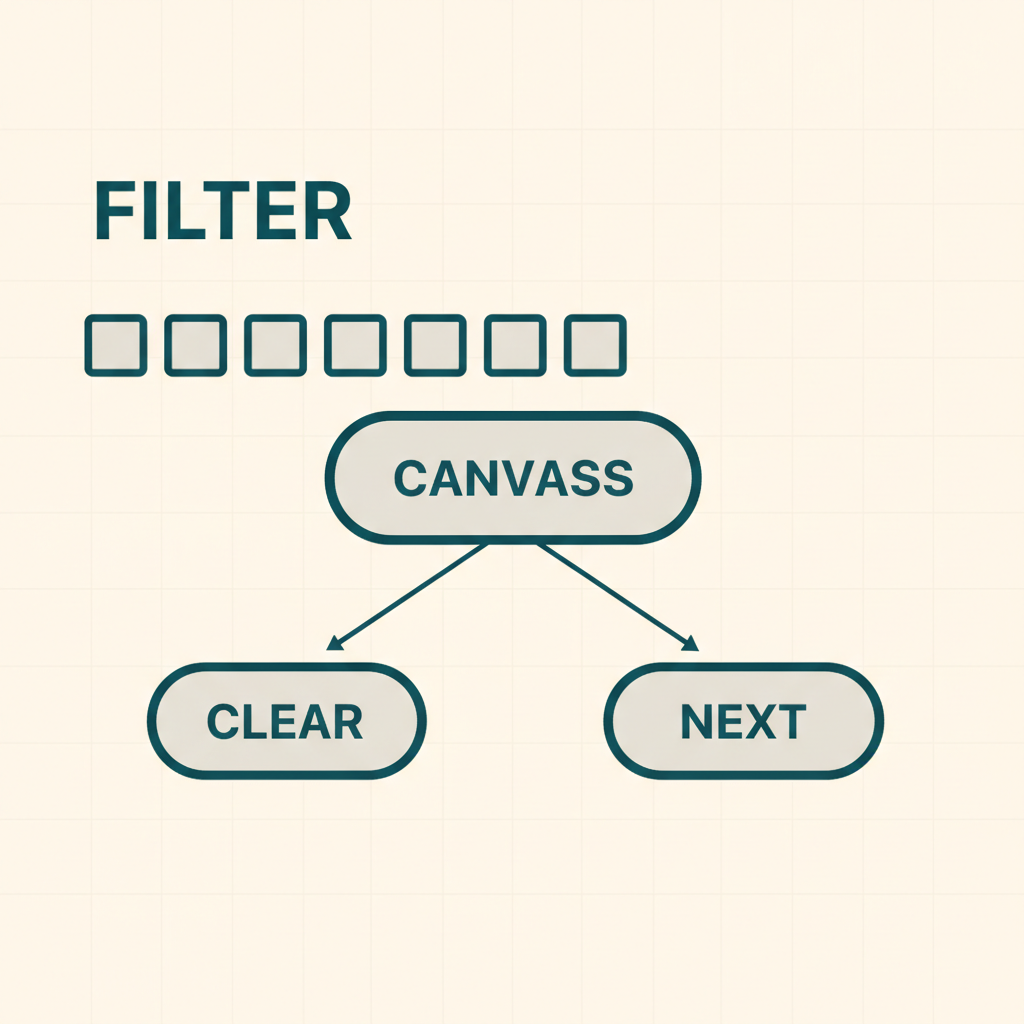
A medical canvass rarely ends an investigation by itself. It produces confirmation, and confirmation either resolves the question an adjuster started with or points to the next investigative step. Alpine Intel frames the canvass as a desktop inquiry that sits early in the stack, ahead of more invasive and more expensive tools.
When a canvass comes back clean, it closes the inquiry. The claimant's reported history matches what facilities confirmed, no undisclosed prior treatment surfaces, and the adjuster can advance the claim with documented support. That outcome matters as much as a hit. A negative canvass is evidence the claim checks out, not a dead end.
When a canvass surfaces something, Alpine Intel names three pathways an adjuster can take from there. The first is a medical authorization request for full records, which is the natural follow-up when canvass results show treatment the claimant never disclosed and the adjuster needs the clinical detail behind it. The second is a subpoena, used when a facility will not release records voluntarily or the claimant declines to sign an authorization. The third is a referral to an investigator for surveillance, social media investigation, or a background check, which fits cases where the canvass raises behavioral red flags rather than documentation gaps.
Each pathway escalates cost, time, and intrusiveness, so the canvass earns its place by filtering which cases deserve that escalation. An adjuster who orders surveillance on every soft-tissue claim burns budget on claims that would have cleared. A canvass run first tells you which claims justify the spend. That sequencing is what makes canvassing a screening layer rather than a standalone answer, and it keeps the heavier tools reserved for the claims that actually warrant them.
What to Look for in a Medical Canvassing Vendor
CDI Canvassing frames its methodology around four attributes worth borrowing as evaluation criteria, even if you never hire CDI. The labels are predictable, reliable, repeatable, and scalable. Translate each into a question you put directly to a vendor.
Predictable means the vendor runs the same workflow on every file. Ask how they scope geography and facility lists, and whether two different canvassers working the same claim would produce the same outreach plan. A vendor that improvises case by case will hand you inconsistent results that fall apart when an adjuster or defense counsel scrutinizes them.
Reliable comes down to documentation. Ask what the vendor delivers when a facility confirms treatment and what it delivers when a facility reports no record. Verbal confirmations that never make it into writing cannot support a claim decision. You want documented responses with facility names, contact records, dates, and the specific answer each provider gave.
Repeatable is the standardized methodology question. If a vendor handles your single high-stakes file the same way it handles a routine soft-tissue claim, you can trust the output regardless of stakes. Ask to see a sample canvass report so you can judge the structure rather than the sales pitch.
Scalable matters most for SIU programs that refer canvasses in volume. Ask whether the vendor's outreach can absorb a sudden batch of referrals without turnaround degrading, and how that capacity is built. A vendor staffed entirely by phone agents hits a ceiling the moment your referral count spikes.
Beyond CDI's four attributes, three operational markers separate a rigorous provider from a commodity one. First, facility scope and pharmacy coverage. Alpine Intel canvasses hospitals, urgent care, specialty clinics, and pharmacies within a radius of where the claimant lives or where the injury occurred. A vendor that skips pharmacy canvassing misses prescription pickup records, which often surface treatment a claimant never mentioned.
Second, turnaround accountability. Ask whether the vendor commits to a turnaround window and reports against it, or whether files simply close whenever they close. Early canvassing only reduces downstream rework if results arrive while the claim is still in play.
Third, audit trail output. Every confirmed and negative response should arrive as a record you can hand to an examiner, an adjuster, or counsel without reconstructing what happened. A canvass you cannot defend in documentation is a canvass you cannot use.
How Superunit Supports Medical Canvassing Programs
A medical canvassing program has three operational bottlenecks: scoping the right facilities, reaching all of them fast enough to matter, and producing documentation that holds up downstream. Superunit's AI agents address all three directly.
In a traditional canvassing program, expanding a search radius from 2 miles to 5 miles to 10 miles meaningfully increases the workload — more facilities means more calls, more time, and more staff. With Superunit, radius size does not change turnaround time. The AI agents contact every facility in the defined scope simultaneously, so a broader search costs nothing extra in time. That means canvassers can default to a wider net without tradeoffs, which directly improves hit rate.
The same logic applies to volume. Whether a canvass involves 10 facilities or 1,000, Superunit places all outreach simultaneously across phone, email, and fax, regardless of time zone or business hours. A human team hits a ceiling the moment referral volume spikes. A new client onboards, a fraud sweep generates a batch of referrals, or a staffing gap opens up, and turnaround degrades. Superunit's AI workforce scales up and down instantly with volume, so seasonal swings and client changes don't create backlogs. The constraint is contact data quality, not capacity.
The documentation side follows the same pattern. Each contact Superunit makes is automatically logged with a timestamp, the outreach method used, a call recording, and a transcript. Confirmed treatments and confirmed negatives both land in the same auditable record. An adjuster receives a complete canvass file rather than a set of notes someone wrote down from memory, so every finding is traceable and defensible if the claim is contested or escalated to litigation.
Superunit does not replace the judgment a canvass feeds. An adjuster still decides whether findings warrant a medical authorization, surveillance, or closing the inquiry. What it removes is the labor bottleneck and documentation inconsistency between referral and result.
Frequently Asked Questions
How is a medical canvass different from medical records retrieval?
A canvass confirms whether treatment occurred and when and where, without pulling charts, billing statements, or clinical notes. Records retrieval requires a signed authorization or subpoena and returns the full file. You order a canvass to map the treatment landscape, then request records only for the facilities worth a closer look.
Does a canvass require patient authorization?
No. A canvass surfaces only non-protected details such as dates of service, provider identity, and whether treatment happened, which HIPAA permits a facility to confirm without a release. The moment you need diagnoses, notes, or billing detail, you cross into protected information that does require authorization or a subpoena.
When in the claims lifecycle should a canvass be ordered?
Early, before the claim direction hardens. CDI Canvassing argues that earlier canvassing reduces downstream delays and rework, and that timing holds in practice. A canvass run in the first weeks shapes investigation strategy, while one ordered after months of activity mostly confirms what you already paid to learn.
What happens if the canvass turns up undisclosed treatment?
Undisclosed treatment opens the next investigative step rather than resolving the claim by itself. Depending on the finding, you can issue a subpoena, request full records through a medical authorization, or refer the file to an investigator for surveillance or a social media review. A documented canvass result gives each of those steps a defensible starting point.
How long does a medical canvass take?
Turnaround depends on the geographic radius, the number of facilities contacted, and how quickly providers respond, so a tight local canvass clears faster than a multi-state sweep. Vendors rarely publish fixed timelines because facility response speed varies widely. Ask any vendor to commit to a turnaround range and to report negative responses, not just hits, so you know the canvass actually covered the scope you ordered.